The Science Behind Gender-Affirming Care for Minors

Jon Stewart (L) and Leslie Rutledge (R), the Arkansas Attorney General [2].
Jon Stewart recently released an interview with Arkansas Attorney General Leslie Rutledge, pushing back on her state’s passing of Act 626 [1]. Act 626 is the first bill in the nation to ban gender-affirming care, such as hormones, puberty blockers, and surgeries, for minors. While Stewart has long served as a staunch left-wing figure, a new and mounting body of evidence suggests that the scientific position lies in supporting Act 626.
Opponents of the bill argue that gender-affirming care is crucial to prevent depression and suicide in transgender youth [3]. The current research is not strong enough to support this claim. One study associated gender-affirming treatment with much lower odds of depression and suicide [4]. However, according to a supplemental table of outcomes over time, the rates hardly change. From baseline to 12 months, depression rates decrease only from 57% to 56%, anxiety from 57% to 51%, and suicidal thoughts from 43% to 37%. The evidence that such care meaningfully improves mental health outcomes is sparse. After considering over 100 follow-up studies of transgender individuals, the Guardian did not find a study that provides rigorous evidence and evaluation that gender-affirming care helps patients [5]. Small sample sizes, lost participants, and skewed design plagues most of such studies. A 2019 article published in the American Journal of Psychiatry provided data that time since gender-affirming surgery was associated with reduced mental health treatment, but a 2020 correction found no advantage of surgery in relation to other forms of mental health treatment [6][7]. The study also could not find a significant effect of hormone treatment on the use of mental health treatment. When closely examined, the benefits of gender-affirming care become less apparent.
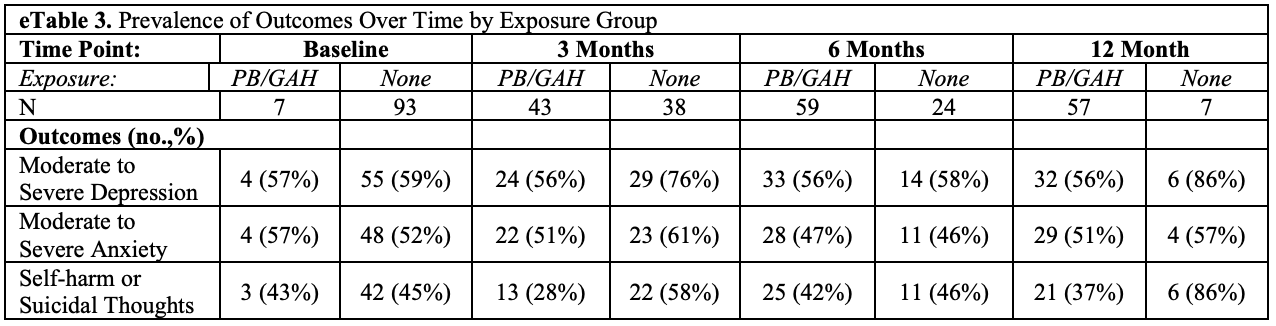
Table from Tordoff 2022, Supplemental Content, e-Table 3 [4].
Opponents of the bill also argue that gender-affirming care is reversible [3]. This position used to be pervasive, even having appeared on the British NHS website, but emerging data paints a more nuanced picture [8]. Updates to the NHS website acknowledge that the long-term side effects of gender-affirming treatment are poorly understood, and that they may even affect the growth of the brain and the bones [9]. The website also now recognizes the irreversible aspects of hormone treatment, such as breast and vocal development. They may even cause potentially irreversible infertility. The NHS represents a foreign perspective, but the science abroad is still applicable to US policy. Across the Atlantic, the US Department of Health and Human Services’ Office of Population Affairs takes an ambiguous position and lists hormone therapy as “partially reversible,” which skirts details about the risks of undergoing treatment [10]. One study published in mid-2022 discusses another newly-discovered side effect: pseudotumor cerebri, a buildup of pressure in the brain [11]. With healthcare issues, politics should follow science. If the updated science raises questions about the safety and reversibility of gender-affirming treatment, doctors and parents should perhaps avoid prescribing them to children. If scientists are only beginning to understand the effects of hormone treatment, it is unreasonable to expect children to fully understand the implications of their decision.
The fact that scientists have not yet fully investigated the effects of gender-affirming care raises the question of whether children can truly consent to such treatment. Not only do children’s decision-making abilities not fully develop until adulthood, gender-dysphoric children are significantly more likely to be diagnosed with depression, anxiety, ADHD, and autism [12][13][14]. Children with these mental health issues would struggle even more than mentally healthy children to grasp the implications of their decision to undertake gender-affirming care. Children who suffer from anxiety and depression already struggle with understanding reality and making judgements and decisions, and the decision to undertake gender-affirming care is no different. In practice, children do not make the decision alone, but with the aid of parents and doctors. Do doctors help these children make the right decision?
Unfortunately, doctors and clinics often neglect to provide adequate evaluation of their dysphoric patients before beginning treatment. A study of 100 detransitioners in the United States found that over half of them believed that doctors failed to provide a thorough evaluation before starting treatment [15]. Mental health professionals in the United States and abroad have clearly failed to take the time to fully assess patients to ensure that gender-affirming care is the correct treatment.

The now-closed Tavistock Centre in London [16].
Keira Bell represents one of many gender-dysphoric children who no longer remain dysphoric after puberty after being treated at the Tavistock Centre in London. One study of dysphoric children found that, of the 54 children who followed up, only 21 remained dysphoric, while 33 became no longer dysphoric after approximately ten years [17]. An older study assessed 139 boys from ages 3 to 13 and followed up 13 to 40 years later, classifying only 17 of them as “persisters” who continued to have gender dysphoria [18]. Another study placed the rate of desisters at 84% by adolescence or adulthood [19]. Clearly, beginning treatment in childhood would include large numbers of children who would no longer be dysphoric in adulthood. Those who remain dysphoric should absolutely pursue treatment. However, given the huge commitment and risks of puberty blockers, hormone replacement therapy, and surgery, doctors should only initiate these treatments on those who will remain dysphoric.
Other countries have already noted the issues with gender-affirming care and have codified precautions. In Sweden in 2021, the children’s hospital of the Karolinska Institute, a medical research giant, chose to prohibit hormone treatment in children under age sixteen [20]. For children between 16 and 18, the hospital requires approval from an ethical review agency and a rigorous assessment of the child’s ability to understand the consequences of treatment.
A 2022 statement by the NHS acknowledged that gender dysphoria “may be a transient phase,” citing the Endocrine Society’s Clinical Practice Guidelines: “combining all outcome studies to date, the gender dysphoria / gender incongruence of a minority of prepubertal children appears to persist in adolescence [21].” The Endocrine Society is a worldwide community of researchers and doctors. The NHS statement also advises precautions on the use of puberty blockers until further research is completed: “NHS England will only commission GnRHa in the context of a formal research protocol.” Act 626 would not descend the US into conservativism, but bring the US closer to the updated science and in line with other developed countries.
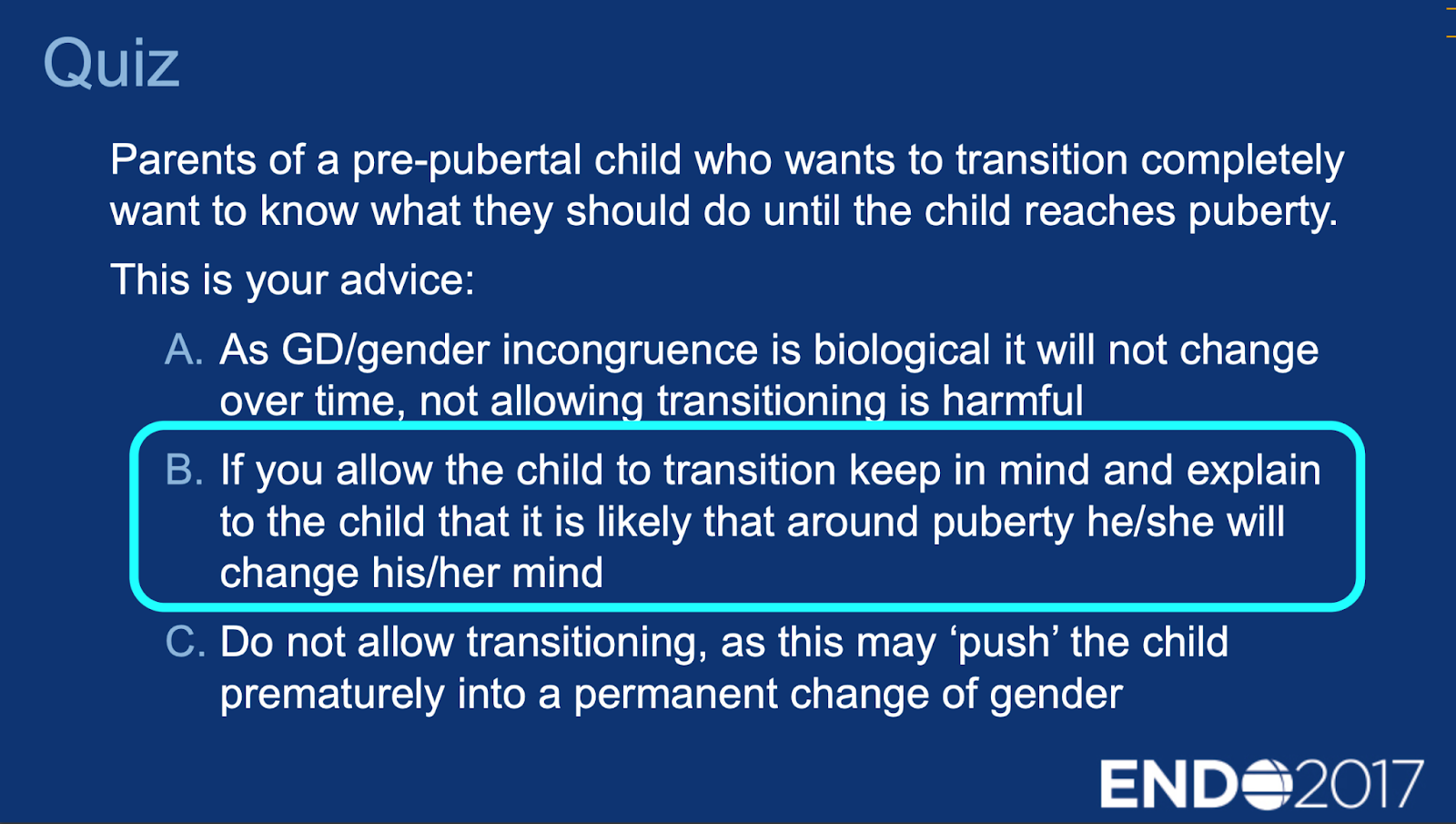
Slide from the Endocrine Society Educational Slide Deck Acknowledging High Likelihood of Gender Dysphoria Reversal among Children [22].
The staggering rate of children who lose their gender dysphoria after puberty should not be a surprise. The evidence paints a picture of dysphoric children with higher rates of depression and autism who are rushed to start puberty blockers and hormone therapy without proper evaluation, most of whom would lose their gender dysphoria over their lifetimes. Gender-affirming care is an expensive, lifelong, and life-changing process that should only be performed on people who will remain dysphoric past puberty. Once on hormone treatment, the children may feel like their bodies more closely match their self-perception, but they may also suffer irreversible, dangerous, and unexpected effects to their brains, bones, and sexual organs. Because the science has yet to settle, it is impossible for dysphoric children to make an informed choice and understand the risks of undergoing treatment. The current system is not a case of children rationally and carefully choosing to undergo reversible care after evaluation. The current system is doctors hastily prescribing irreversible and poorly-understood treatment to children, most of whom would not stop being dysphoric at some point in their lives.
Act 626 bans gender-affirming care for minors in Arkansas—the first such bill in the nation to do so. Such a ban addresses many of the problems with the transgender care system outlined in this article. The ban allows more time for the decision-making faculties of dysphoric children to develop and gives them more time to understand the positive and negative effects of hormone treatment. The ban also prevents clinics from rushing to start puberty blockers and hormone therapy, allowing them time to conduct a full psychiatric evaluation of children. More thorough examinations would likely prevent cases of dysphoric children who would later change their mind from taking the next step in treatment and regretting it later. A voter that values science and evidence should support Act 626, because the bill places controls on an otherwise poorly-understood and regulated medical system. The bill also updates the law with the most current understanding of hormone therapy, which is not completely safe and fully reversible, but more complex and nuanced, requiring greater care and understanding from doctors and patients before use. Act 626 would bring US policy in line with the NHS, Karolinska Institute, the Endocrine Society, and numerous peer-reviewed papers. Politicians frequently disagree and change laws and guidelines, but the science distinctly supports Act 626.
Sources
1. “Watch The War Over Gender - The Problem With Jon Stewart (Season 2, Episode 1) | Apple TV+.” 2022. Apple TV. October 6, 2022. https://tv.apple.com/us/episode/the-war-over-gender/umc.cmc.1jj39s607lehulo4k0iscsarp?showId=umc.cmc.4fcexvzqezr25p9weks6sxpob.
2. Factora, James. 2022. “Jon Stewart’s Take Down of Arkansas’ Transphobic Policies Is a Must-Watch.” Them. October 10, 2022. https://www.them.us/story/jon-stewart-interview-transphobic-politician.
3. Yurcaba, Jo. 2021. “Arkansas Passes Bill to Ban Gender-Affirming Care for Trans Youth.” NBC News. March 29, 2021. https://www.nbcnews.com/feature/nbc-out/arkansas-passes-bill-ban-gender-affirming-care-trans-youth-n1262412.
4. Tordoff, Diana M., Jonathon W. Wanta, Arin Collin, Cesalie Stepney, David J. Inwards-Breland, and Kym Ahrens. 2022. “Mental Health Outcomes in Transgender and Nonbinary Youths Receiving Gender-Affirming Care.” JAMA Network Open 5 (2): e220978. https://doi.org/10.1001/jamanetworkopen.2022.0978.
5. Batty, David. 2004. “Mistaken Identity | Health | The Guardian.” The Guardian. July 30, 2004. https://www.theguardian.com/society/2004/jul/31/health.socialcare.
6. Bränström, Richard, and John E. Pachankis. 2020. “Reduction in Mental Health Treatment Utilization Among Transgender Individuals After Gender-Affirming Surgeries: A Total Population Study.” American Journal of Psychiatry 177 (8): 727–34. https://doi.org/10.1176/appi.ajp.2019.19010080.
7. “Correction to Bränström and Pachankis.” 2020. American Journal of Psychiatry 177 (8): 734–734. https://doi.org/10.1176/appi.ajp.2020.1778correction.
8. “Gender Dysphoria - Treatment (Wayback Machine).” 2020. NHS. May 2, 2020. https://web.archive.org/web/20200502223746/https:/www.nhs.uk/conditions/gender-dysphoria/treatment/.
9. “Gender Dysphoria - Treatment.” 2020. NHS. May 28, 2020. https://www.nhs.uk/conditions/gender-dysphoria/treatment/.
10. Office of Population Affairs. n.d. “Gender-Affirming Care and Young People,” 2.
11. Food and Drug Administration. 2022. “Risk of Pseudotumor Cerebri Added to Labeling for Gonadotropin-Releasing Hormone Agonists,” July 1, 2022. https://publications.aap.org/aapnews/news/20636/Risk-of-pseudotumor-cerebri-added-to-labeling-for.
12. “The Teen Brain: 7 Things to Know.” n.d. National Institute of Mental Health (NIMH). Accessed November 27, 2022. https://www.nimh.nih.gov/health/publications/the-teen-brain-7-things-to-know.
13. Mulrooney, Lindsey. 2022. “Study: Transgender Children at Higher Risk for Mental Health Problems.” Pharmacy Times. August 2, 2022. https://www.pharmacytimes.com/view/study-transgender-children-at-higher-risk-for-mental-health-problems.
14. Warrier, Varun, David M. Greenberg, Elizabeth Weir, Clara Buckingham, Paula Smith, Meng-Chuan Lai, Carrie Allison, and Simon Baron-Cohen. 2020. “Elevated Rates of Autism, Other Neurodevelopmental and Psychiatric Diagnoses, and Autistic Traits in Transgender and Gender-Diverse Individuals.” Nature Communications 11 (1): 3959. https://doi.org/10.1038/s41467-020-17794-1.
15. Littman, Lisa. 2021. “Individuals Treated for Gender Dysphoria with Medical and/or Surgical Transition Who Subsequently Detransitioned: A Survey of 100 Detransitioners.” Archives of Sexual Behavior 50 (8): 3353–69. https://doi.org/10.1007/s10508-021-02163-w.
16. BBC News. 2021. “The Crisis at the Tavistock’s Child Gender Clinic,” March 30, 2021, sec. UK. https://www.bbc.com/news/uk-56539466.
17. Wallien, Madeleine S. C., and Peggy T. Cohen-Kettenis. 2008. “Psychosexual Outcome of Gender-Dysphoric Children.” Journal of the American Academy of Child & Adolescent Psychiatry 47 (12): 1413–23. https://doi.org/10.1097/CHI.0b013e31818956b9.
18. D, Singh, Bradley Sj, and Zucker Kj. 2021. “A Follow-Up Study of Boys With Gender Identity Disorder.” Frontiers in Psychiatry 12 (March). https://doi.org/10.3389/fpsyt.2021.632784.
19. Steensma, Thomas D., Jenifer K. McGuire, Baudewijntje P. C. Kreukels, Anneke J. Beekman, and Peggy T. Cohen-Kettenis. 2013. “Factors Associated With Desistence and Persistence of Childhood Gender Dysphoria: A Quantitative Follow-Up Study.” Journal of the American Academy of Child & Adolescent Psychiatry 52 (6): 582–90. https://doi.org/10.1016/j.jaac.2013.03.016.
20. Astrid Lindgren Children’s Hospital. 2021. “Policy Change Regarding Hormonal Treatment of Minors with Gender Dysphoria at Tema Barn - Astrid Lindgren Children’s Hospital,” April 1, 2021. https://segm.org/sites/default/files/Karolinska%20_Policy_Statement_English.pdf
21. “Specialist Service for Children and Young People with Gender Dysphoria (Phase 1 Providers).” 2022. NHS England. https://www.engage.england.nhs.uk/specialised-commissioning/gender-dysphoria-services/user_uploads/b1937-ii-specialist-service-for-children-and-young-people-with-gender-dysphoria-1.pdf.
22. “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons.” 2017. JAMA 318 (15): 1491. https://doi.org/10.1001/jama.2017.13540.